![]()
Beautiful Plants For Your Interior
Ethylmorphine, recognized by its alternative names codethyline and dionine, originated as a semi-synthetic morphinan opioid, initially synthesized by Merck in the year 1884. It was developed as a milder substitute for morphine. In contemporary times, its primary application lies in its role as an antitussive agent. Ethylmorphine is commonly found in cough syrup formulations like Cocillana, Cosylan, Solvipect comp. (often combined with guaifenesin), and Lepheton (typically paired with ephedrine). Alternatively, it is available in tablet form under the brand name Tussipax, often combined with codeine. Notably, cough syrup formulations often include a gentle laxative to mitigate constipation, a common side effect of opioids.
Ethylmorphine also finds utility in ophthalmic preparations, where it is referred to as dionine, serving to address ocular inflammations. In the year 1904, a preparation containing ethylmorphine was introduced as a novel ocular analgesic.
| Identifiers | |
|---|---|
| IUPAC name | |
| CAS Number | 76-58-4 |
|---|---|
| PubChem CID | 5359271 |
| DrugBank | DB01466 |
| ChemSpider | 4514250 |
| UNII | RWO67D87EU |
| KEGG | D07929 |
| CompTox Dashboard (EPA) | DTXSID1046760 |
| ECHA InfoCard | 100.000.883 |
| Chemical and physical data | |
| Formula | C19H23NO3 |
| Molar mass | 313.397 g·mol−1 |
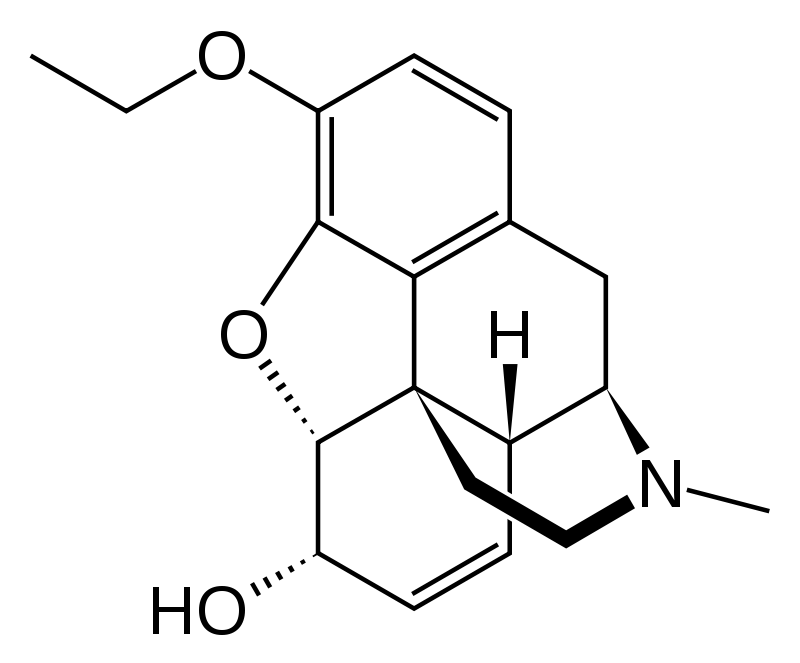
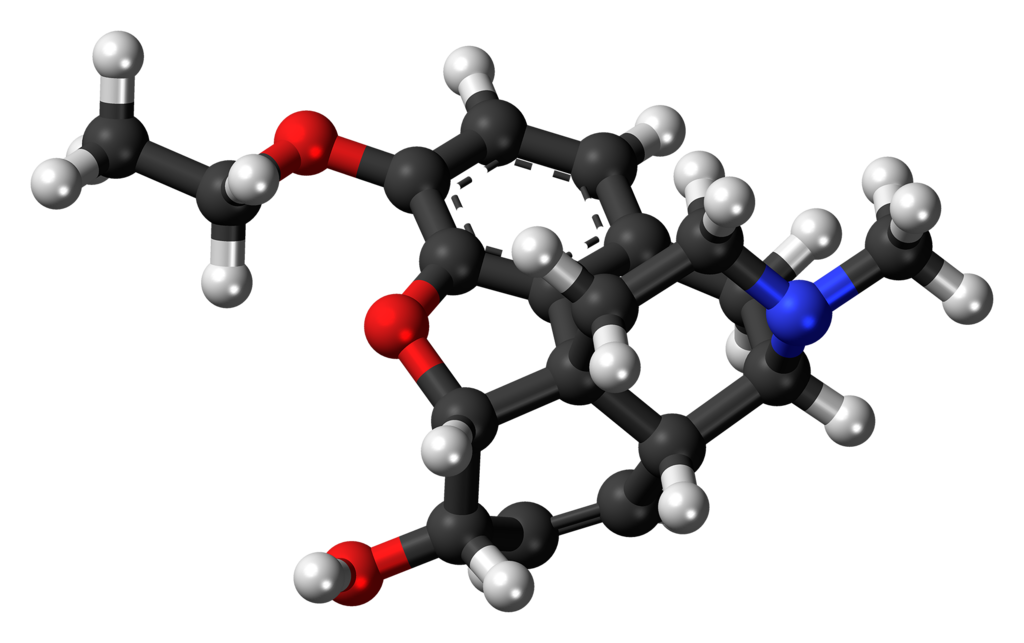
Ethylmorphine, also known as 3-ethylmorphine, belongs to the morphinan class of opioids. Within this class, ethylmorphine and similar compounds share a complex molecular framework consisting of three interconnected benzene rings arranged in a zig-zag fashion referred to as phenanthrene. Additionally, a fourth ring containing nitrogen is fused to the phenanthrene structure at positions R9 and R13, with the nitrogen atom being situated at position R17 within this composite structure. This distinctive configuration is commonly known as a morphinan.
In the case of ethylmorphine and its fellow morphinans, an ether bridge is formed between two of these rings, specifically linking positions R4 and R5 through an oxygen atom. Furthermore, ethylmorphine features a hydroxy group (OH-) attached at position R6 and a methyl group located on the nitrogen atom at position R17. On the same ring housing the hydroxy group, ethylmorphine shares a double bond with codeine and morphine.
Ethylmorphine bears a close relationship to morphine, as both compounds possess an oxygen group at position R3. However, in ethylmorphine, this oxygen group is substituted with an ethyl group, resulting in an ethoxy group. Notably, ethylmorphine’s distinction from naturally occurring codeine (3-methylmorphine) is characterized by the presence of an ethoxy group in place of the methoxy group, making them homologous compounds. Additionally, ethylmorphine shares structural similarities with other morphinans, including dihydrocodeine, heroin, hydrocodone, and oxycodone.
The active metabolites derived from ethylmorphine, notably morphine, exert their actions by binding to and activating the μ-opioid receptor. This phenomenon occurs because opioids possess a structural resemblance to endogenous endorphins, which naturally occur in the body and also engage with the μ-opioid receptor system. This structural similarity between opioids and endorphins underlies the experience of euphoria, pain relief, and anxiolysis when opioids are used. This is because endorphins play a crucial role in alleviating pain, inducing drowsiness, and generating feelings of pleasure. These endorphins can be released in response to various stimuli, including pain, strenuous physical activity, orgasm, or heightened excitement.
It’s worth noting that ethylmorphine has been described as having less potency than morphine but slightly greater potency than codeine.
Disclaimer: The following effects are based on the Subjective Effect Index (SEI), which relies on anecdotal user reports and personal analyses contributed by PsychonautWiki collaborators. It is advisable to approach these effects with a healthy degree of skepticism.
It’s also important to note that these effects may not necessarily manifest predictably or consistently. Higher doses are more likely to encompass the full range of effects, while escalating doses increase the risk of adverse outcomes, including addiction, severe harm, or even fatality ☠.
Ethylmorphine exhibits a comparatively low level of toxicity in relation to its dosage. Nevertheless, despite its relatively low toxicity for an opioid, there has been at least one documented fatality attributed to the sole oral consumption of ethylmorphine without the presence of other depressants. Like all opioids, long-term usage can result in varying effects, including reduced libido, apathy, and memory impairment. It can also prove fatal when combined with depressants such as alcohol or benzodiazepines.
It is highly advisable to implement harm-reduction strategies when using this substance.
As with other opioids, the chronic use of ethylmorphine can lead to a high potential for abuse and psychological dependence among certain individuals. Once addiction has taken hold, individuals may experience cravings and withdrawal symptoms if they abruptly discontinue usage.
Tolerance to many of the effects of ethylmorphine develops over time with repeated use. The rate at which tolerance develops can vary for different effects, with tolerance to constipation-inducing effects developing particularly slowly, for instance. Consequently, users may find themselves needing to administer increasingly higher doses to achieve the same effects. After discontinuation, it typically takes about 3 to 7 days for the tolerance to decrease by half and 1 to 2 weeks to return to baseline (in the absence of further consumption). Ethylmorphine also presents cross-tolerance with all other opioids, meaning that after consuming ethylmorphine, the effectiveness of all opioids will be reduced.
Warning: Many psychoactive substances that are reasonably safe when used individually can suddenly become hazardous and even life-threatening when combined with certain other substances. The following list highlights some known dangerous interactions (though it may not cover all possibilities).
It is crucial to conduct independent research (e.g., using resources like Google, DuckDuckGo, and PubMed) to ensure that combining two or more substances is safe. Some of the interactions listed below have been sourced from TripSit.
Generally, due to their structural and pharmacological similarities, ethylmorphine and codeine are subject to similar legal regulations in most countries.
1. What is Ethylmorphine?
Ethylmorphine is an opioid analgesic medication used for the relief of pain and as a cough suppressant. It belongs to the class of drugs known as opioids and is structurally similar to codeine.
2. How does Ethylmorphine work?
Ethylmorphine acts on the central nervous system to relieve pain and suppress coughing. It binds to specific receptors in the brain and spinal cord, ultimately reducing the perception of pain and cough reflex sensitivity.
3. Is Ethylmorphine available over the counter?
The availability of Ethylmorphine varies by country and region. In some places, you may be able to purchase certain formulations containing Ethylmorphine without a prescription, while in others, it may require a prescription.
4. What are the common medical uses of Ethylmorphine?
Ethylmorphine is primarily used as a cough suppressant to alleviate dry, non-productive coughs. It may also be prescribed for pain relief in some cases.
5. Are there any potential side effects of Ethylmorphine?
Yes, like other opioids, Ethylmorphine can cause side effects, including drowsiness, dizziness, constipation, nausea, and, in some cases, respiratory depression. It’s essential to take it as prescribed and under medical supervision.
6. Can Ethylmorphine be habit-forming or addictive?
Yes, Ethylmorphine has a potential for abuse and addiction, especially with prolonged use or misuse. Individuals may develop tolerance and dependence, leading to cravings and withdrawal symptoms upon discontinuation.
7. Can I drink alcohol while taking Ethylmorphine?
It is generally not recommended to consume alcohol while taking Ethylmorphine, as both substances can have central nervous system depressant effects. Combining them can increase the risk of dangerous side effects and respiratory depression.
8. Is Ethylmorphine safe during pregnancy and breastfeeding?
Ethylmorphine should only be used during pregnancy or breastfeeding under the guidance of a healthcare professional. It can pass into breast milk and potentially harm a nursing infant.
9. Can Ethylmorphine interact with other medications or substances?
Yes, Ethylmorphine can interact with other medications, especially those that have central nervous system depressant effects. It’s important to inform your healthcare provider about all the drugs and substances you are taking to avoid potentially harmful interactions.
10. Is it safe to drive or operate heavy machinery while taking Ethylmorphine?
Ethylmorphine can cause drowsiness and impaired coordination. It is not safe to drive or operate machinery while under the influence of Ethylmorphine, especially if you are not familiar with its effects on your body.
11. Can I suddenly stop taking Ethylmorphine if I’ve been using it for a while?
No, abruptly discontinuing Ethylmorphine after prolonged use can lead to withdrawal symptoms. It’s crucial to taper off the medication under medical supervision to minimize discomfort and health risks.
12. How should I store Ethylmorphine?
Store Ethylmorphine as directed on the prescription label or by your pharmacist. Typically, it should be kept at room temperature, away from moisture, heat, and direct sunlight.
13. What should I do if I suspect an overdose of Ethylmorphine?
An overdose of Ethylmorphine can be life-threatening. If you suspect an overdose or experience symptoms like extreme drowsiness, slow breathing, or loss of consciousness, seek immediate medical attention or call emergency services.
14. Can I share my Ethylmorphine prescription with someone else?
No, it is not safe or legal to share prescription medications with others. Ethylmorphine should only be used by the individual for whom it was prescribed under the supervision of a healthcare provider.
15. Where can I find more information about Ethylmorphine?
For specific information about Ethylmorphine, its uses, and potential risks, consult your healthcare provider pharmacist or refer to the medication’s package insert. Always rely on trusted medical sources for accurate information.