![]()
Beautiful Plants For Your Interior
Diphenhydramine, known by various names such as DPH, Dimedrol, and Benadryl, among others, belongs to the ethanolamine class and is classified as a deliriant substance. It falls into the category of first-generation H1 antihistamines and is widely available as an over-the-counter medication for managing allergies. When consumed in excess of recommended doses, diphenhydramine can induce potent delirium.
This compound was initially synthesized in 1943 and gained approval as the first prescription antihistamine by the U.S. Food and Drug Administration in 1946. Subsequently, in the 1980s, it was cleared for over-the-counter use. Presently, diphenhydramine finds common application in allergy relief, but it may also be prescribed for addressing conditions like itchiness, insomnia, motion sickness, nausea, and symptoms associated with Parkinson’s disease.
Subjective effects of diphenhydramine encompass sedation, anxiety, tactile hallucinations, memory impairment, thought disarray, dysphoria, and external hallucinations. Lower doses tend to elicit a calming, bodily relaxation, whereas higher doses induce a state of deliriousness, featuring vivid and compelling hallucinations. Dosages falling in between these two extremes often lead to discomfort and dysphoria.
Notably, many users report significant nausea and physical discomfort, often referred to as “body load.” A majority of individuals who experiment with diphenhydramine do not describe positive effects and do not seek to repeat the experience.
This substance is generally considered to have a low potential for abuse due to its unpleasant effects. The toxicological implications of recreational use have not been extensively researched. Anecdotal accounts suggest that chronic use, characterized by high doses and repeated consumption, may result in persistent hallucinations and impairments in cognitive function and memory. High doses have also been associated with seizures and cardiac toxicity.
It is highly advisable to prioritize harm-reduction practices when using this substance.
| Identifiers | |
|---|---|
| IUPAC name | |
| CAS Number | 58-73-1 |
|---|---|
| PubChem CID | 3100 |
| IUPHAR/BPS | 1224 |
| DrugBank | DB01075 |
| ChemSpider | 2989 |
| UNII | 8GTS82S83M |
| KEGG | D00300 |
| ChEBI | CHEBI:4636 |
| ChEMBL | ChEMBL657 |
| CompTox Dashboard (EPA) | DTXSID4022949 |
| ECHA InfoCard | 100.000.360 |
| Chemical and physical data | |
| Formula | C17H21NO |
| Molar mass | 255.361 g·mol−1 |
George Rieveschl, a former professor at the University of Cincinnati, discovered Diphenhydramine in 1943. In 1946, it achieved the distinction of becoming the first prescription antihistamine to gain approval from the United States Food and Drug Administration (FDA).
During the 1960s, it was uncovered that diphenhydramine could inhibit the reuptake of the neurotransmitter serotonin. This significant finding prompted a quest to identify potential antidepressants that shared similar structural traits while having fewer associated side effects. This research ultimately led to the development of fluoxetine (Prozac), a selective serotonin reuptake inhibitor (SSRI).
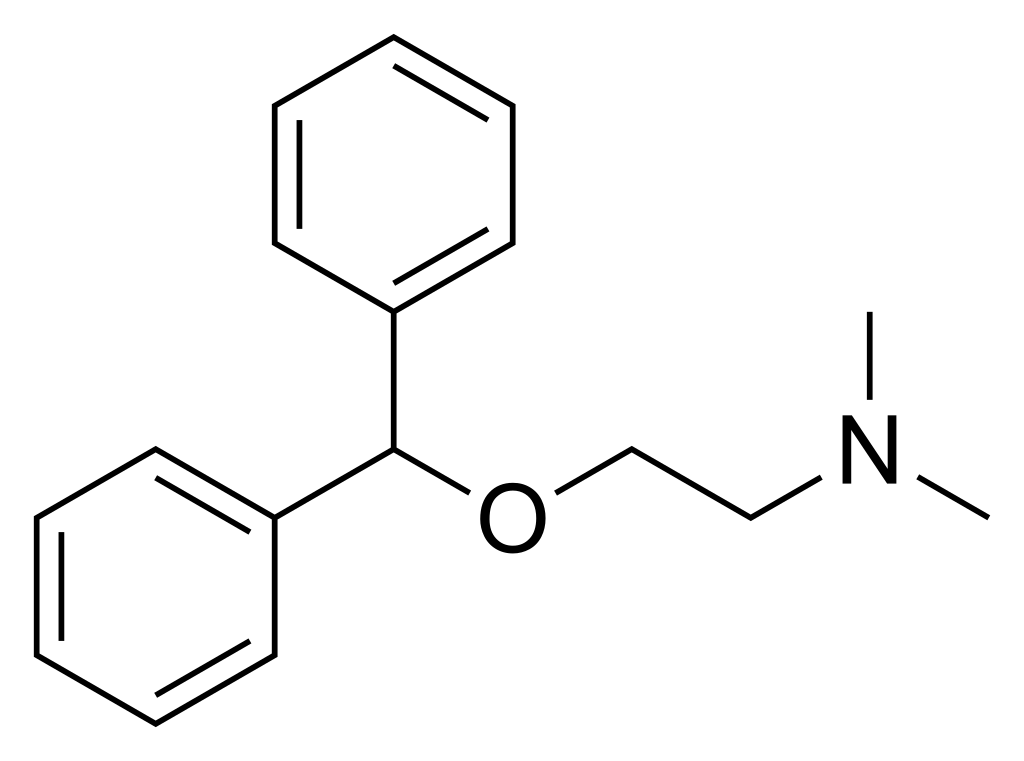
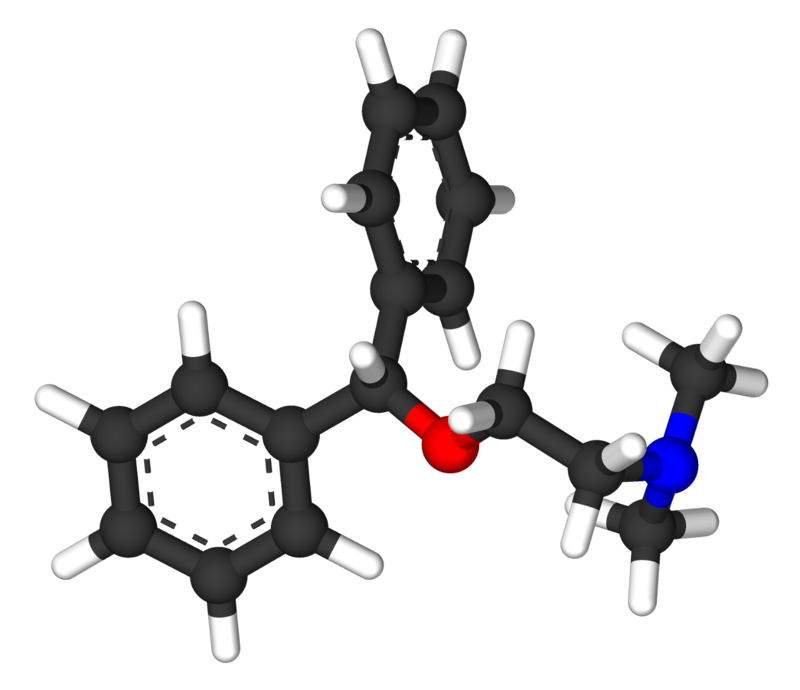
Diphenhydramine, scientifically known as 2-(diphenylmethoxy)-N, N-dimethylethanamine, falls within the category of organic compounds belonging to the ethanolamine class. Its chemical structure comprises an ethylamine chain that contains two methyl groups attached to the end nitrogen atom RN. Furthermore, this ethylamine chain carries a substitution at R2 in the form of a diphenylmethoxy group, creating an ether linkage. The diphenylmethoxy group consists of two aromatic phenyl rings joined to a carbon atom that is also linked to a methoxy group CH3O-.
Diphenhydramine is commonly manufactured in the form of a hydrochloride salt.
Diphenhydramine functions as an inverse agonist at both the peripheral histamine receptor and the central histamine receptor, which is supported by references.[citation needed] Its peripheral inverse agonistic activity contributes to its allergy-alleviating effects. Additionally, like many first-generation antihistamines, it competes with acetylcholine receptors (mACH receptors) as a competitive antagonist.
Diphenhydramine serves as an antagonist of acetylcholine receptors. While the exact mechanism remains not entirely understood, it is believed that the inhibition of acetylcholine’s actions primarily accounts for the development of delirium, sedation, and vividly realistic hallucinations, along with the highly uncomfortable and dysphoric physical side effects.
Moreover, studies have indicated that diphenhydramine can block sodium channels and impede serotonin reuptake. It also hinders voltage-gated potassium channels (VGKCs), potentially giving rise to or contributing to the development of torsades de pointes. This potentially hazardous cardiac condition can lead to sudden cardiac death.
The receptor binding affinities are detailed as follows:
| Receptor Site | Binding Affinity (nM, Lower = Stronger) |
|---|---|
| H1 | 9.6-16 |
| H2 | missing data |
| H3 | >10,000 |
| H4 | >10,000 |
| M1 | 80-100 |
| M2 | 120-490 |
| M3 | 84-299 |
| M4 | 53-112 |
| M5 | 30-260 |
| SERT | ≥3,800 |
According to user accounts, Diphenhydramine exhibits a non-linear dose-response pattern, meaning that its effects do not directly correlate with the dosage. Doses below 300 mg are said to induce restlessness, muscle relaxation, and a body high, while amounts surpassing 500 mg start to lead to a state of delirium, characterized by vivid and convincingly realistic hallucinations. Doses falling in between these two extremes are described as uncomfortable and dysphoric, often accompanied by nausea and bodily discomfort, commonly referred to as “body load.”
Please note that the following effects are based on the Subjective Effect Index (SEI), which relies on anecdotal user reports and personal observations of PsychonautWiki contributors. Therefore, they should be approached with a degree of skepticism.
It’s essential to be aware that these effects may not occur predictably or consistently, and higher doses are more likely to produce the full range of products. Additionally, higher doses can lead to adverse outcomes, including addiction, severe injury, or even death ☠.
The potential risks and long-term health consequences of recreational diphenhydramine use have not undergone extensive study.
Diphenhydramine can be highly unpredictable, and its mechanism for inducing hallucinations carries the risk of causing severe harm, hospitalization, or even fatality. Moreover, it places users in a state where they have limited control over their actions, potentially leading to bizarre and nonsensical behavior that puts the user in jeopardy.
Reports from individuals suggest that regular use of diphenhydramine may have severe repercussions for kidney and bladder health, similar to the issues observed in ketamine cystitis cases.
There is tentative evidence linking cumulative diphenhydramine use to an elevated risk of developing dementia.
The commonly accepted overdose threshold for diphenhydramine is around 1000 milligrams; however, susceptible individuals or those using other substances concurrently can overdose with smaller amounts. Overdosing on diphenhydramine leads to effects similar to those of heavy doses, including delirium, psychosis, anxiety, confusion, increased heart rate,[citation needed], elevated blood pressure[citation needed], dryness, urinary retention, dizziness, and dilated pupils. At very high doses, more severe side effects may occur, including the risk of seizures,[citation needed], and dangerous cardiovascular effects like arrhythmia (abnormal heartbeat).
The user may lose the ability to distinguish reality from hallucinations, creating a substantial risk of responding to delusional perceptions and causing harm to themselves or others. There is also the possibility of excessive physical activity, which can strain the heart or lead to rhabdomyolysis. In cases of delusion, individuals should, if possible, be kept calm. The primary treatment for overdose should involve the administration of benzodiazepines, although immediate medical attention is crucial.
Fatalities can occur with doses of diphenhydramine that come close to or exceed 2 grams.[citation needed] This risk increases significantly when combined with most stimulants, depressants, and MAOIs.
User reports suggest that diphenhydramine induces psychosis and delirium at a notably higher rate than other hallucinogens (such as psychedelics and dissociatives).[citation needed] Numerous online experience reports describe states of psychotic rage, amnesia, and other serious consequences following misuse of the substance. In many instances, these outcomes have led to hospitalization and even death.
Diphenhydramine can lead to dependence with chronic use. Compared to other hallucinogens, DPH is reported to have significantly less abuse potential, primarily because the majority of people who try it do not desire to repeat the experience.
Tolerance to many of the effects of DPH develops with repeated use, necessitating increasingly larger doses to achieve the same impact. After discontinuation, it takes approximately 1 to 2 weeks for tolerance to return to baseline (in the absence of further consumption). DPH also presents cross-tolerance with all deliriants, meaning that after consuming DPH, all deliriants will have a reduced effect.
Warning: Many psychoactive substances that are relatively safe when used independently can become dangerous and even life-threatening when combined with certain other substances. The following list highlights some known dangerous interactions (although it may not encompass all of them).
Always conduct thorough independent research (e.g., through Google, DuckDuckGo, or PubMed) to ensure that a combination of two or more substances is safe to consume. Some of the interactions listed have been sourced from TripSit.
1. What is diphenhydramine? Diphenhydramine is an antihistamine medication that is commonly used to treat allergies. It is also known by brand names such as Benadryl and has some off-label uses, including as a sleep aid.
2. How does diphenhydramine work? Diphenhydramine works by blocking the effects of histamine, a chemical that your body releases during an allergic reaction. By blocking histamine, it can relieve allergy symptoms like sneezing, runny nose, itching, and watery eyes.
3. Is diphenhydramine available over the counter? Yes, diphenhydramine is available over the counter without a prescription in many countries. It is commonly found in allergy relief medications, sleep aids, and as a standalone product.
4. Can I use diphenhydramine as a sleep aid? Yes, diphenhydramine is often used as a sleep aid due to its soothing effects. However, it’s essential to follow the recommended dosage guidelines and consult with a healthcare professional, as long-term or excessive use may have adverse effects.
5. What are the potential side effects of diphenhydramine? Common side effects of diphenhydramine include drowsiness, dry mouth, dizziness, blurred vision, and constipation. It can also cause more severe side effects, such as an allergic reaction, difficulty breathing, or a rapid heart rate. If you experience severe side effects, seek medical attention immediately.
6. Can diphenhydramine be abused recreationally? Yes, some individuals misuse diphenhydramine for its hallucinogenic effects, especially at higher doses. However, recreational use is not advised due to the potential for serious health risks and adverse effects.
7. What are the dangers of recreational diphenhydramine use? Recreational use of diphenhydramine can lead to hallucinations, confusion, delirium, and other severe psychological and physical effects. Overdosing on diphenhydramine can be life-threatening and may cause cardiac problems, seizures, and psychosis.
8. Is diphenhydramine addictive? Diphenhydramine has the potential for dependence with chronic use, but it is generally considered to have low abuse potential compared to other substances. Most people who try it do not wish to repeat the experience.
9. Can diphenhydramine interact with other medications? Yes, diphenhydramine can interact with other medicines, including certain antidepressants, sedatives, and drugs that affect the central nervous system. It’s essential to consult with a healthcare professional before combining diphenhydramine with other medications.
10. Is diphenhydramine safe for everyone to use? Diphenhydramine may not be safe for individuals with certain medical conditions, such as glaucoma, enlarged prostate, or asthma. Pregnant or nursing women should consult with a healthcare provider before using it. Always follow the recommended dosages and guidelines on the product label.
11. Can I drive or operate heavy machinery while using diphenhydramine? Diphenhydramine can cause drowsiness and impair cognitive function, so it’s essential to avoid activities that require alertness, such as driving or operating machinery, until you know how it affects you.
12. Where can I get more information about diphenhydramine? For specific questions or concerns about diphenhydramine, it’s best to consult with a healthcare professional or pharmacist. They can provide personalized guidance based on your medical history and needs.
1. Emanuel, M. B. (July 1999). “Histamine and the antiallergic antihistamines: a history of their discoveries: History of antiallergic antihistamines”. Clinical & Experimental Allergy. 29: 1–11. This publication explores the history of antiallergic antihistamines, shedding light on the discovery and development of drugs like diphenhydramine. It provides valuable insights into the early understanding of histamine and its role in allergies.
2. Drugs.com – Diphenhydramine Hydrochloride This online resource offers comprehensive information on diphenhydramine hydrochloride, including its uses, dosages, side effects, and precautions. It’s a valuable reference for those seeking detailed information on this medication.
3. Jang, D. H., Manini, A. F., Trueger, N. S., Duque, D., Nestor, N. B., Nelson, L. S., Hoffman, R. S. (November 2010). “Status epilepticus and wide-complex tachycardia secondary to diphenhydramine overdose”. Clinical Toxicology. 48 (9): 945–948. This study discusses a severe case of status epilepticus and tachycardia resulting from a diphenhydramine overdose. It highlights the importance of understanding the potential dangers of excessive diphenhydramine use.
4. Hevesi D (29 September 2007). “George Rieveschl, 91, Allergy Reliever, Dies”. The New York Times. This New York Times article commemorates George Rieveschl, the inventor of diphenhydramine. It provides insights into his contributions to allergy relief and the pharmaceutical industry.
5. “Benadryl”. Ohio History Central. Ohio History Central offers historical information on Benadryl, shedding light on its origins and development. It’s a useful resource for understanding the history of this well-known antihistamine.
6. Ritchie J (24 September 2007). “UC prof, Benadryl inventor dies”. Business Courier of Cincinnati. This article discusses the passing of George Rieveschl, the inventor of Benadryl, and his legacy. It provides information on his academic and scientific achievements.
7. Domino EF (1999). “History of modern psychopharmacology: a personal view with an emphasis on antidepressants”. Psychosomatic Medicine. 61 (5): 591–8. This publication offers a personal perspective on the history of modern psychopharmacology, including insights into the development of antidepressants like diphenhydramine.
8. Awdishn RA, Whitmill M, Coba V, Killu K (October 2008). “Serotonin reuptake inhibition by diphenhydramine and concomitant linezolid use can result in serotonin syndrome”. Chest. 134 (4 Meeting abstracts). This study discusses the potential for serotonin syndrome resulting from the combination of diphenhydramine and linezolid. It highlights the importance of understanding drug interactions.
9. Khalifa, M., Drolet, B., Daleau, P., Lefez, C., Gilbert, M., Plante, S., O’Hara, G. E., Gleeton, O., Hamelin, B. A., Turgeon, J. (February 1999). “Block of potassium currents in guinea pig ventricular myocytes and lengthening of cardiac repolarization in man by the histamine H1 receptor antagonist diphenhydramine”. The Journal of Pharmacology and Experimental Therapeutics. 288 (2): 858–865. This study explores the effects of diphenhydramine on potassium currents in cardiac cells, shedding light on its potential impact on cardiac repolarization.
10. Kim, Y. S., Shin, Y. K., Lee, C., Song, J. (27 October 2000). “Block of sodium currents in rat dorsal root ganglion neurons by diphenhydramine”. Brain Research. 881 (2): 190–198. This study investigates how diphenhydramine affects sodium currents in rat dorsal root ganglion neurons, providing insights into its mechanisms of action.
11. Thakur, A. C., Aslam, A. K., Aslam, A. F., Vasavada, B. C., Sacchi, T. J., Khan, I. A. (15 February 2005). “QT interval prolongation in diphenhydramine toxicity”. International Journal of Cardiology. 98 (2): 341–343. This publication discusses the QT interval prolongation associated with diphenhydramine toxicity, highlighting the potential cardiac effects of overdose.
12. Lilienfield, L. S., Rose, J. C., Princiotto, J. V. (April 1976). “Antitussive activity of diphenhydramine in chronic cough”. Clinical Pharmacology and Therapeutics. 19 (4): 421–425. This study explores the antitussive (cough-suppressing) activity of diphenhydramine, offering insights into its potential uses beyond allergy relief.
13. Hou, R. H., Scaife, J., Freeman, C., Langley, R. W., Szabadi, E., Bradshaw, C. M. (June 2006). “Relationship between sedation and pupillary function: comparison of diazepam and diphenhydramine”. British Journal of Clinical Pharmacology. 61 (6): 752–760. This research investigates the relationship between sedation and pupillary function, comparing the effects of diazepam and diphenhydramine.
14. Putra, Okky Dwichandra; Yoshida, Tomomi; Umeda, Daiki; Higashi, Kenjirou; Uekusa, Hidehiro; Yonemochi, Etsuo (29 July 2016). “Crystal Structure Determination of Dimenhydrinate after More than 60 Years: Solving Salt–Cocrystal Ambiguity via Solid-State Characterizations and Solubility Study”. Crystal Growth & Design. 16 (9): 5223–5229. This study delves into the crystal structure determination of dimenhydrinate, a salt form of diphenhydramine, providing insights into its physical properties.
15. “Dimenhydrinate injection, solution”. Daily Med. U.S. National Library of Medicine. Daily Med offers information on dimenhydrinate injection, providing details on its formulation and usage.
16. Gray, S. L., Anderson, M. L., Dublin, S., Hanlon, J. T., Hubbard, R., Walker, R., Yu, O., Crane, P. K., Larson, E. B. (March 2015). “Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study”. JAMA internal medicine. 175 (3): 401–407. This comprehensive study investigates the relationship between the cumulative use of strong anticholinergic drugs (including diphenhydramine) and the incidence of dementia.
17. Emadian, S. M., Caravati, E. M., Herr, R. D. (October 1996). “Rhabdomyolysis: a rare adverse effect of diphenhydramine overdose”. The American Journal of Emergency Medicine. 14 (6): 574–576. This research discusses a rare adverse effect of diphenhydramine overdose: rhabdomyolysis, which involves the breakdown of muscle tissue.
18. Erowid Diphenhydramine (Benadryl) Vault: Legal Status Erowid provides information on the legal status of diphenhydramine, offering insights into its regulatory status in various regions.