Flunitrazepam is a potent and sedative medication commonly known by the brand name “Rohypnol.” Although it’s primarily used for treating severe insomnia and certain medical conditions, it has also gained notoriety as a recreational drug, often referred to as a “date rape drug.” This duality has led to concerns regarding its accessibility through various channels, including online vendors and research chemical sellers.
Research chemical sellers have found a niche market in providing substances like Flunitrazepam. They often market it as a “designer drug” or a “research chemical,” which can be misleading and potentially dangerous. While some individuals may genuinely seek these substances for research purposes, most likely buy them for recreational use or self-medication, often without a clear understanding of the risks involved.
One of the primary issues with online Flunitrazepam sellers is the lack of regulation and oversight. Unlike pharmaceutical companies, these vendors often operate in a legal grey area, making selling potentially harmful substances to unsuspecting buyers easier. This lack of leadership means that the quality, purity, and dosage of Flunitrazepam purchased online can vary significantly, putting consumers at risk of overdose or adverse reactions.
Furthermore, the marketing tactics employed by these sellers can be misleading and irresponsible. They may downplay the potential dangers of Flunitrazepam, leading buyers to underestimate the risks associated with its use. Such practices endanger individuals’ health and safety and contribute to the drug’s misuse and abuse.
Contents
- 1 Summary
- 2 History and culture
- 3 Chemistry
- 4 Pharmacology
- 5 Subjective effects
- 6 Toxicity
- 7 Legal status
- 8 FAQ
- 8.1 1. What is Flunitrazepam?
- 8.2 2. What are some familiar brand names for Flunitrazepam?
- 8.3 3. Is Flunitrazepam legal?
- 8.4 4. What are the common uses of Flunitrazepam?
- 8.5 5. Is Flunitrazepam safe to use?
- 8.6 6. What are the potential side effects of Flunitrazepam?
- 8.7 7. Can Flunitrazepam be abused?
- 8.8 8. Is Flunitrazepam available over-the-counter (OTC)?
- 8.9 9. Can Flunitrazepam be used long-term?
- 8.10 10. How should Flunitrazepam be taken?
- 8.11 11. Can I drink alcohol while taking Flunitrazepam?
- 8.12 12. What should I do if I miss a dose of Flunitrazepam?
- 8.13 13. Is Flunitrazepam safe during pregnancy and breastfeeding?
- 8.14 14. Can I stop taking Flunitrazepam abruptly?
- 8.15 15. Where can I get more information about Flunitrazepam?
- 9 References
Summary
Flunitrazepam, commercially known as Rohypnol, belongs to the benzodiazepine class of depressant substances. When administered, it primarily induces hypnotic and amnesic effects while exhibiting anxiolytic, anticonvulsant, and sedative properties.
Hoffmann-La Roche first synthesized Flunitrazepam in 1972. In certain countries, it finds application for short-term insomnia treatment and as a preoperative sedative. Remarkably, it boasts a potency approximately tenfold greater than diazepam when comparing equivalent weights.
Users must be aware that abruptly discontinuing benzodiazepine use can pose significant risks, potentially even life-threatening, especially for individuals who have been using them regularly over extended periods. This abrupt cessation can lead to severe outcomes, such as seizures or even fatal consequences. Therefore, it is highly recommended that individuals adopt a tapering approach, gradually reducing their daily dose over an extended period instead of ceasing usage suddenly.
| Identifiers | |
|---|---|
| show IUPAC name | |
| CAS Number | 1622-62-4 |
| PubChem CID | 3380 |
| IUPHAR/BPS | 4193 |
| DrugBank | DB01544 |
| ChemSpider | 3263 |
| UNII | 620X0222FQ |
| KEGG | D01230 |
| ChEBI | CHEBI:31622 |
| ChEMBL | ChEMBL13280 |
| CompTox Dashboard (EPA) | DTXSID7023065 |
| ECHA InfoCard | 100.015.089 |
| Chemical and physical data | |
| Formula | C16H12FN3O3 |
| Molar mass | 313.288 g·mol−1 |
History and culture
Flunitrazepam, originally discovered within Roche’s benzodiazepine research program under the leadership of Leo Sternbach, made its debut in the market in 1974 and was introduced to the European commercial market in 1975 under the trade name Rohypnol. During the 1980s, its availability expanded to other countries.
Notably, it gained notoriety as the date-rape drug Rohypnol, commonly called “roofie.” In response to the drug’s widespread misuse for recreational and illicit purposes, Roche took action in 1998. They modified the 1 mg tablets to reduce their solubility and incorporated a blue dye, making it easier to detect when added to beverages.
Research conducted in Sweden revealed that flunitrazepam ranked as the second most frequently encountered drug in suicides, present in approximately 16% of cases. In a retrospective study of 1,587 deaths in Sweden, benzodiazepines were implicated in 159 instances. Notably, in suicides involving benzodiazepines, flunitrazepam and nitrazepam were found in significantly higher concentrations than natural deaths.
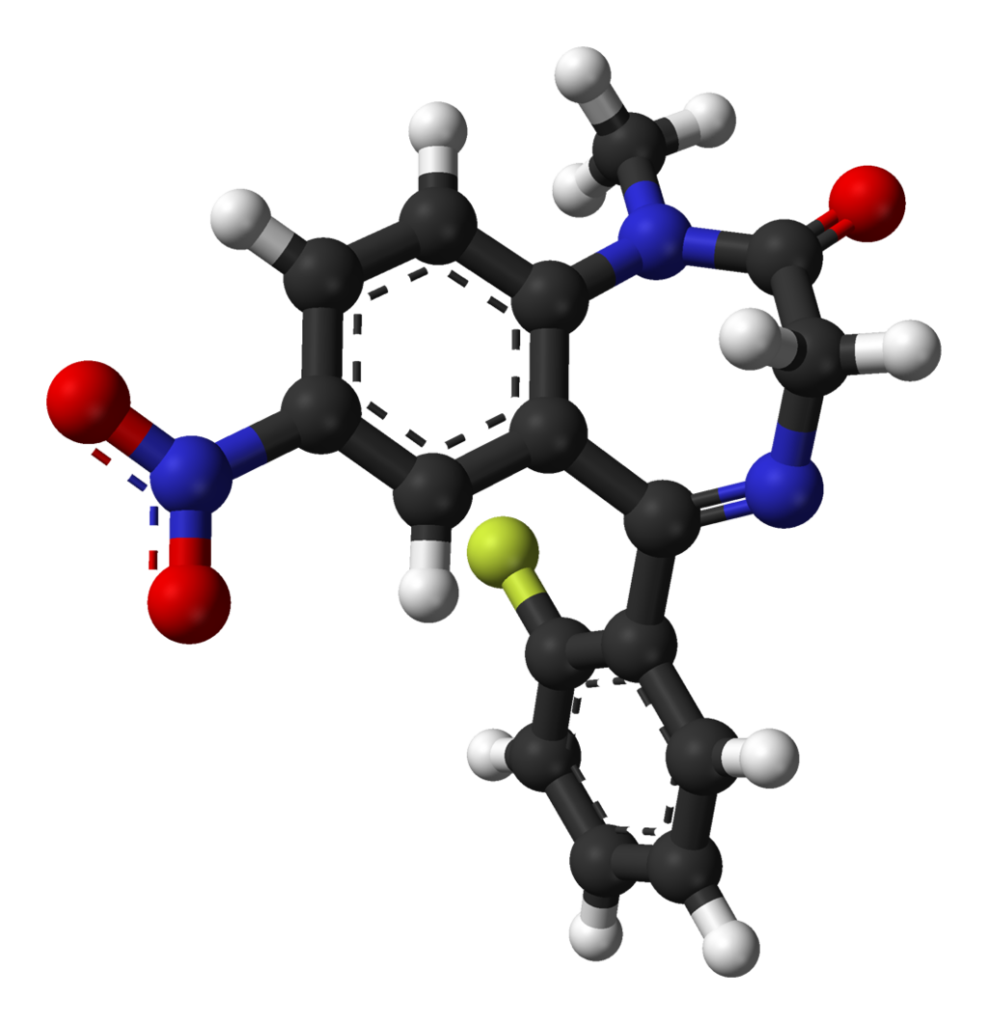
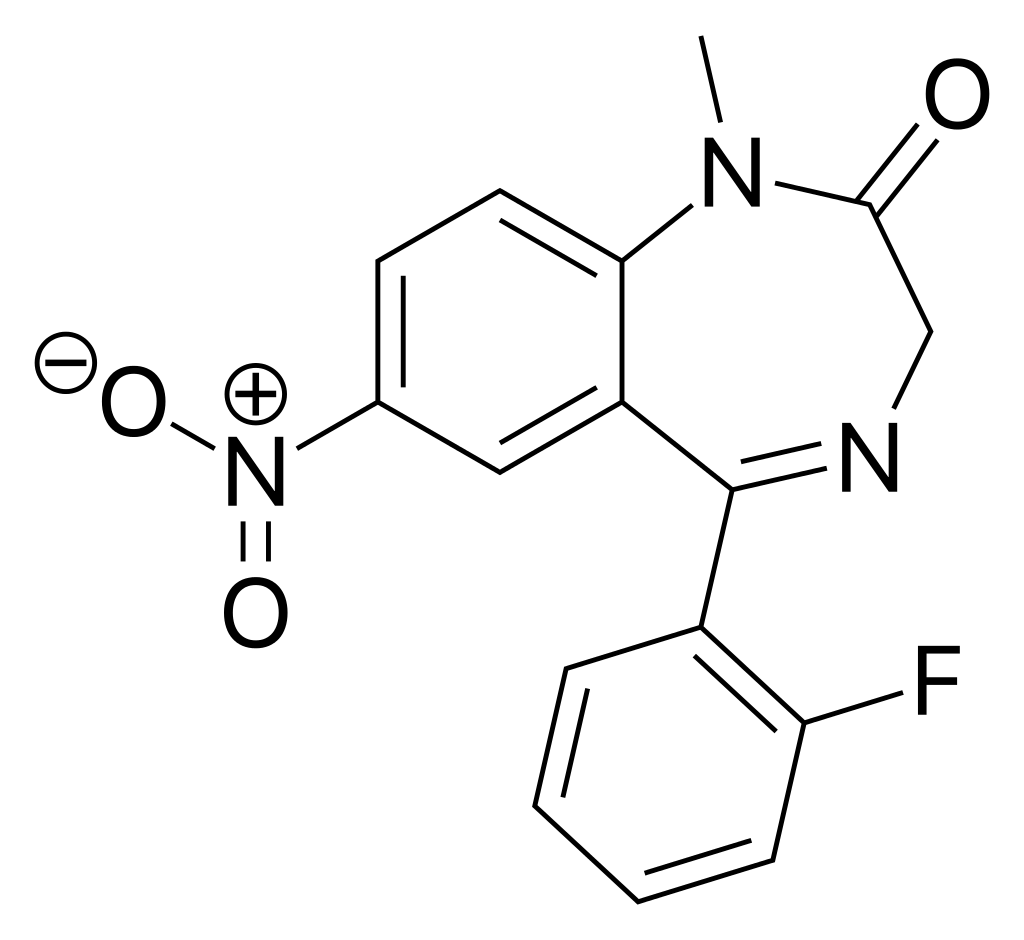
Chemistry
Flunitrazepam belongs to the nitro-benzodiazepine class of compounds. It is derived from nitrazepam through fluorination of the N-methyl group. Within this category, other nitro-benzodiazepines include nitrazepam, which serves as the parent compound, nimetazepam, a methylamino derivative, and clonazepam, characterized by a 2ʹ-chlorinated modification.
Pharmacology
Benzodiazepines exert a diverse range of effects by binding to the benzodiazepine receptor site, which enhances the efficiency and impact of the neurotransmitter gamma-aminobutyric acid (GABA) by interacting with its receptors. Given that this receptor site is prominently associated with inhibition in the brain, the modulation of this system results in Flunitrazepam’s calming or soothing effects on the nervous system.
It’s worth noting that the anticonvulsant properties of benzodiazepines may, in part or entirely, be attributed to their binding to voltage-dependent sodium channels rather than benzodiazepine receptors.
Flunitrazepam is recognized for its ability to induce anterograde amnesia when administered in sufficient doses, causing individuals to be unable to recollect specific events experienced while under the drug’s influence. This effect can be especially concerning if Flunitrazepam is misused in cases of sexual assault, as victims may struggle to recall the assault, identify the assailant, or remember the circumstances surrounding the incident.
Approximately 80% of orally administered Flunitrazepam is absorbed, while its bioavailability in suppository form is closer to 50%.
Subjective effects
Please be aware that the effects described below are derived from the Subjective Effect Index (SEI), which relies on anecdotal user accounts and the personal assessments of contributors to PsychonautWiki. As a result, it’s essential to approach these effects with a measure of scepticism.
Furthermore, it’s crucial to understand that these effects may not manifest consistently or predictably. Higher doses are more likely to produce full results but also increase the risk of adverse consequences, including addiction, severe harm, or even fatality ☠.
Flunitrazepam is commonly associated with a mental state characterized by intense sedation, drowsiness, relaxation, anxiety relief, memory impairment, and reduced inhibition, akin to the mental state experienced at higher doses of diazepam and temazepam.
Physical:
- Sedation: Flunitrazepam can induce profound sedation, often leading to an overwhelming sense of lethargy. At higher doses, users may feel as if they are severely sleep-deprived, making physical activity challenging and potentially causing complete unconsciousness.
- Dizziness
- Nausea
- Muscle Relaxation
- Loss of Motor Control
- Respiratory Depression
- Suppression of Seizures
- Decreased Heart Rate
- Decreased Blood Pressure
- Perception of Bodily Heaviness: Flunitrazepam can induce a feeling of bodily heaviness, ranging from motor impairment at lower doses to complete lethargy or inability to move at higher doses.
- Physical Euphoria: The euphoria experienced with Flunitrazepam is notably stronger compared to other benzodiazepines like alprazolam.
- Dry Mouth
Paradoxical:
Paradoxical reactions to benzodiazepines, such as increased seizures (in people with epilepsy), aggression, heightened anxiety, violent behaviour, loss of impulse control, irritability, and suicidal tendencies, are rare in the general population (with an incidence rate below 1%). However, they occur more frequently among recreational users, individuals with mental disorders, children, and those on high-dosage regimens.
Cognitive:
The cognitive effects of Flunitrazepam intensify with dosage and include:
- Amnesia: Flunitrazepam can lead to substantial memory impairment.
- Cognitive Euphoria: Cognitive euphoria on Flunitrazepam is significantly more pronounced than that induced by other benzodiazepines like alprazolam.
- Anxiety Suppression
- Thought Deceleration
- Analysis Suppression
- Disinhibition
- Compulsive Redosing
- Emotion Suppression: While primarily reducing anxiety, Flunitrazepam also dampens other emotions to a degree, though less intensively than antipsychotics.
- Delusions of Sobriety: This involves mistakenly believing one is utterly sober despite clear evidence to the contrary, often occurring at higher doses.
- Memory Suppression: Flunitrazepam primarily impairs short-term memory, leading to forgetfulness and disorganized behaviour.
- Confusion: At heavy doses, Flunitrazepam may confuse due to the drug’s suppression of essential cognitive functions such as comprehension, memory, and reasoning.
- Motivation Suppression: The sedation and lethargy induced by Flunitrazepam may make physical activities or efforts challenging, especially at higher doses.
- Language Suppression: Flunitrazepam can result in slurred speech and difficulty communicating clearly.
- Dream Potentiation: While most users report benzodiazepines like Flunitrazepam lead to dreamless sleep, the opposite effect has been noted, particularly during withdrawal from GABAergic substances like alcohol. The reasons for these differences are not fully understood.
After:
- Rebound Anxiety: After taking substances like benzodiazepines that relieve anxiety, users may experience a rebound effect, corresponding to the total duration and amount consumed, potentially fostering dependence and addiction.
- Residual Sleepiness: While benzodiazepines can be effective sleep aids, their effects may linger into the morning, causing users to feel groggy for several hours.
- Dream Potentiation or Dream Suppression
- Residual Sleepiness
- Thought Deceleration
- Thought Disorganization
- Irritability
Please exercise caution when considering Flunitrazepam, and always consult a healthcare professional for guidance. Misuse or abuse of this substance can have severe consequences.
Toxicity
Flunitrazepam is generally considered to have a relatively low toxicity in its dosage. However, it can become lethal with depressants such as alcohol or opioids.
It is strongly advised to practice harm reduction when using this drug.
Lethal Dose:
The oral LD50 (the dose destructive in 50% of the population) of flunitrazepam is 1200 mg/kg in mice and 415 mg/kg in rats.
Tolerance and Addiction Potential Flunitrazepam is highly physically and psychologically addictive.
Tolerance to its sedative-hypnotic effects typically develops within a few days of continuous use. After discontinuation, tolerance usually returns to baseline within 7 to 14 days. However, in some instances, especially with prolonged and intense usage, this process may take considerably longer.
Withdrawal or rebound symptoms may manifest when discontinuing use abruptly after several weeks or more of steady dosing. Gradual dose reduction may be necessary to manage these symptoms safely. For comprehensive guidance on tapering off benzodiazepines in a controlled manner, please refer to this guide.
Discontinuing benzodiazepines is notoriously challenging and can be life-threatening if not done through a gradual tapering process over several weeks. There is an increased risk of hypertension, seizures, and even death during withdrawal, particularly when drugs that lower the seizure threshold, like tramadol, are avoided.
Flunitrazepam induces cross-tolerance with all benzodiazepines, meaning that after its consumption, the effectiveness of all benzodiazepines will be reduced.
Dangerous Interactions While many drugs are safe when taken individually, they can become hazardous, even life-threatening, when combined with other substances. The list below includes some common potentially dangerous combinations but may not cover all possibilities. Independent research is essential to ensure the safety of combining two or more substances before consumption.
Depressants (e.g., 1,4-Butanediol, 2-methyl-2-butanol, alcohol, barbiturates, GHB/GBL, methaqualone, opioids): Combining these substances can lead to dangerous levels of respiratory depression. They potentiate each other’s muscle relaxation, sedation, and amnesia effects, potentially causing sudden loss of consciousness. If this occurs, individuals should attempt to sleep in the recovery position or have a friend assist them.
Dissociatives:
This combination increases the risk of vomiting during unconsciousness and the potential for suffocation. It is advisable to sleep in the recovery position or have assistance if necessary.
Stimulants:
Combining benzodiazepines with stimulants is hazardous due to the risk of excessive intoxication. Stimulants counteract the sedative effects of benzodiazepines, leading to increased disinhibition and other products when the motivation wears off. If combined, it’s crucial to limit benzodiazepine dosing strictly. This combination can also result in severe dehydration if hydration is not monitored.
Overdose Benzodiazepine overdose can occur when taken in large quantities or concurrently with other depressants, particularly GABAergic depressants like barbiturates and alcohol, which work similarly but bind to distinct allosteric sites on the GABAA receptor. This potentiation effect can lead to severe consequences. Benzodiazepines increase the frequency of the chlorine ion pore opening on the GABAA receptor, while barbiturates increase the duration of pore opening. Thus, when both are consumed, the ion pore opens more frequently and stays open longer.
Benzodiazepine overdose is a medical emergency that can result in coma, permanent brain injury, or death if not promptly treated. Symptoms may include thought deceleration, slurred speech, confusion, delusions, respiratory depression, coma, or death. Hospital treatment, often involving flumazenil, a GABAA antagonist, is typically required. However, care remains primarily supportive.
Legal status
Australia: Flunitrazepam is categorized as a Schedule 8 (S8) controlled drug in Australia.
Austria: In Austria, Flunitrazepam is legally available for medical purposes under the Arzneimittelgesetz Österreich (AMG), but its sale or possession without a prescription is illegal as per the Suchtmittelgesetz Österreich (SMG).
Canada: Flunitrazepam is designated as a Schedule I controlled substance in Canada, accessible exclusively by prescription.
Germany: Since November 2011, flunitrazepam has been subject to control under Anlage 3 of the BtMG in Germany, necessitating a specialized prescription for its use.
Switzerland: Flunitrazolam is registered as a controlled narcotic substance in Switzerland, although it is sparingly prescribed for severe cases of sleep disorders. Flunitrazolam tablets are exclusively available in 1mg dosages and are distinguishable by their green and blue colouring, which notably tints the mouth when consumed in a dissolved beverage.
United Kingdom: Flunitrazepam falls under Class C and is listed as a Schedule 4 controlled drug by the Misuse of Drugs Regulations 2001.
United States: Flunitrazepam is classified as a Schedule IV drug under the U.S. Controlled Substances Act; however, it is not used for medical purposes in the United States.
FAQ
1. What is Flunitrazepam?
Flunitrazepam is a medication primarily prescribed for the short-term treatment of severe insomnia and as a pre-anesthetic medication. It belongs to a class of drugs known as benzodiazepines.
2. What are some familiar brand names for Flunitrazepam?
Various brand names, including Rohypnol know Flunitrazepam. It may also be sold under generic names in different countries.
3. Is Flunitrazepam legal?
The legal status of Flunitrazepam varies from country to country. It is available by prescription only in some places, while in others, it may be controlled or even illegal.
4. What are the common uses of Flunitrazepam?
Flunitrazepam is typically prescribed for the short-term treatment of severe insomnia and as a pre-anesthetic medication. It is known for its soothing and muscle-relaxing effects.
5. Is Flunitrazepam safe to use?
Flunitrazepam should only be used under the supervision and guidance of a healthcare professional. Like all benzodiazepines, it carries a risk of dependency and should not be used for extended periods.
6. What are the potential side effects of Flunitrazepam?
Common side effects may include drowsiness, dizziness, and reduced coordination. Less commonly, it can lead to memory problems, confusion, and paradoxical reactions.
7. Can Flunitrazepam be abused?
Flunitrazepam has been associated with misuse and abuse, particularly in recreational settings. It has gained notoriety as a “date-rape drug” due to its potential to impair a person’s memory and judgment when used illicitly.
8. Is Flunitrazepam available over-the-counter (OTC)?
In most countries, Flunitrazepam is not available over-the-counter, and a prescription from a healthcare provider is required to obtain it legally.
9. Can Flunitrazepam be used long-term?
Long-term use of Flunitrazepam is generally discouraged due to the risk of dependency, tolerance, and withdrawal symptoms. It is usually reserved for short-term treatment of specific conditions.
10. How should Flunitrazepam be taken?
Flunitrazepam should be taken exactly as prescribed by a healthcare professional. Typically, it is taken shortly before bedtime to help with insomnia. Do not exceed the recommended dose.
11. Can I drink alcohol while taking Flunitrazepam?
Combining alcohol with Flunitrazepam is not recommended, as it can intensify the sedative effects and increase the risk of adverse reactions and impaired judgment.
12. What should I do if I miss a dose of Flunitrazepam?
If you miss a dose, take it as soon as you remember. However, if it’s close to the time for your next scheduled dose, skip the missed dose and continue with your regular dosing schedule. Do not double the amount to make up for a missed one.
13. Is Flunitrazepam safe during pregnancy and breastfeeding?
Flunitrazepam should be used cautiously during pregnancy and breastfeeding and only if the potential benefits outweigh the risks. It can pass into breast milk and may affect the baby.
14. Can I stop taking Flunitrazepam abruptly?
No, it is not advisable to stop taking Flunitrazepam suddenly, as this can lead to withdrawal symptoms. Please consult with a healthcare professional to gradually taper off the medication when discontinuing its use.
15. Where can I get more information about Flunitrazepam?
For more information about Flunitrazepam, consult your healthcare provider or refer to your country’s official medical sources and drug information websites. Always follow your healthcare provider’s guidance for this medication’s safe and appropriate use.
References
- Mandrioli, R., Mercolini, L., Raggi, M. A. (October 2008). “Analyzing Benzodiazepine Metabolism”. Current Drug Metabolism. 9 (8): 827–844. doi:10.2174/138920008786049258. ISSN 1389-2002.
- Lann, M. A., Molina, D. K. (June 2009). “A Fatal Case of Benzodiazepine Withdrawal”. The American Journal of Forensic Medicine and Pathology. 30 (2): 177–179. doi:10.1097/PAF.0b013e3181875aa0. ISSN 1533-404X.
- Kahan, M., Wilson, L., Mailis-Gagnon, A., Srivastava, A. (November 2011). “Canadian Guideline for Safe Benzodiazepine Tapering”. Canadian Family Physician. 57 (11): 1269–1276. ISSN 0008-350X.
- Flunitrazepam – TripSit Wiki (2022).
- Robertson, M. D., Drummer, O. H. (May 1995). “Postmortem Drug Metabolism by Bacteria”. Journal of Forensic Sciences. 40 (3): 382–386. ISSN 0022-1198.
- Haefely, W. (29 June 1984). “Benzodiazepine Interactions with GABA Receptors”. Neuroscience Letters. 47 (3): 201–206. doi:10.1016/0304-3940(84)90514-7. ISSN 0304-3940.
- McLean, M. J., Macdonald, R. L. (February 1988). “Benzodiazepines’ Impact on Spinal Cord Neurons”. The Journal of Pharmacology and Experimental Therapeutics. 244 (2): 789–795. ISSN 0022-3565.
- Saïas, T., Gallarda, T. (September 2008). “Paradoxical Aggressive Reactions to Benzodiazepine Use: A Review”. L’Encephale. 34 (4): 330–336. doi:10.1016/j.encep.2007.05.005. ISSN 0013-7006.
- Paton, C. (December 2002). “Benzodiazepines and Disinhibition: A Review”. Psychiatric Bulletin. 26 (12): 460–462. doi:10.1192/pb.26.12.460. ISSN 0955-6036.
- Bond, A. J. (1 January 1998). “Drug-Induced Behavioral Disinhibition”. CNS Drugs. 9 (1): 41–57. doi:10.2165/00023210-199809010-00005. ISSN 1179-1934.
- Drummer, O. H. (February 2002). “Benzodiazepines – Effects on Human Performance and Behavior”. Forensic Science Review. 14 (1–2): 1–14. ISSN 1042-7201.
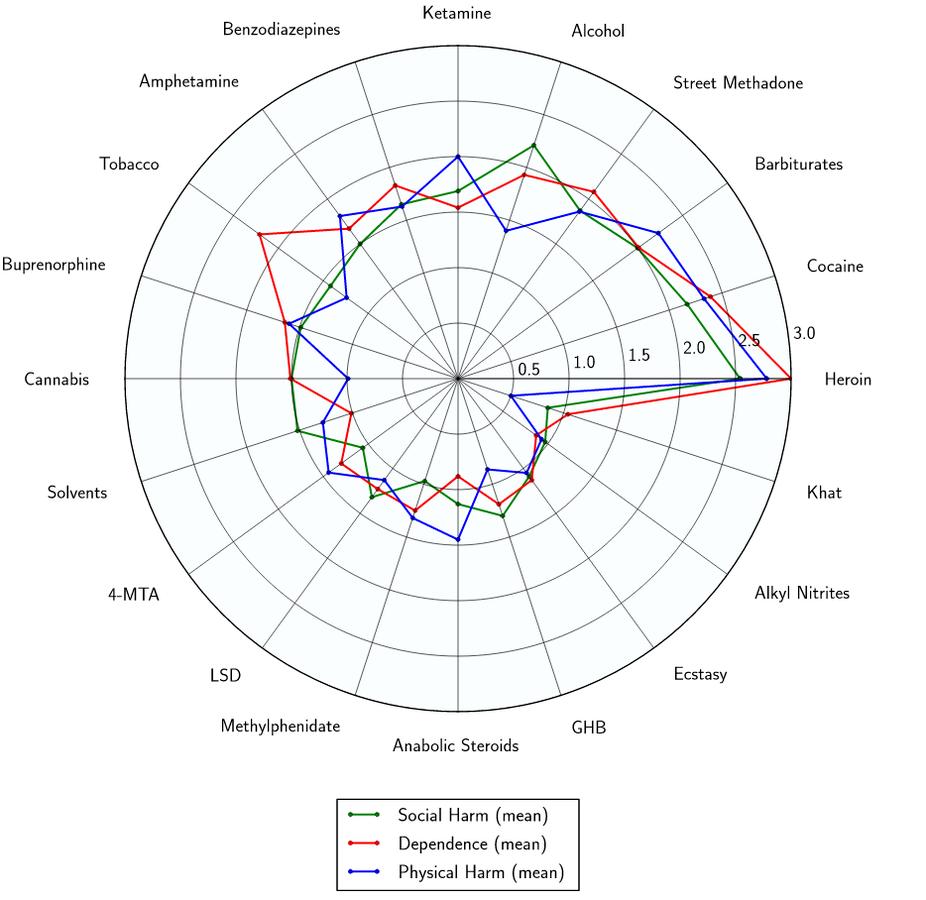
- Nutt, D., King, L. A., Saulsbury, W., Blakemore, C. (24 March 2007). “Harm Assessment of Drugs of Potential Misuse”. The Lancet. 369 (9566): 1047–1053. doi:10.1016/S0140-6736(07)60464-4. ISSN 0140-6736.
- Twyman, R. E., Rogers, C. J., Macdonald, R. L. (March 1989). “Regulation of GABA Receptor Channels by Diazepam and Phenobarbital”. Annals of Neurology. 25 (3): 213–220. doi:10.1002/ana.410250302. ISSN 0364-5134.
- Hoffman, E. J., Warren, E. W. (September 1993). “Flumazenil: A Benzodiazepine Antagonist”. Clinical Pharmacy. 12 (9): 641–656; quiz 699–701. ISSN 0278-2677.
- Controlled Drugs List – UK Government (https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/164222/controlled-drugs-list.pdf).