![]()
Beautiful Plants For Your Interior
Morphine belongs to the morphinan class of naturally occurring opioid substances. It is one of the alkaloids naturally found in opium, derived from the poppy plant Papaver somniferum, alongside codeine. Furthermore, morphine serves as the prototype opiate, setting the standard against which other opioids are measured, including codeine, diacetylmorphine (commonly known as heroin), and hydrocodone.
The isolation of morphine from opium is credited to Friedrich Sertürner, a German pharmacist’s assistant, who achieved this breakthrough in 1806.
Morphine’s subjective effects encompass sedation, pain relief, cough suppression, and euphoria. However, it carries potentially severe side effects, notably respiratory depression and low blood pressure, which can prove fatal when combined with other depressants. Additional side effects include drowsiness, vomiting, and constipation.
The primary source of morphine production involves isolating it from the poppy straw of the opium poppy plant.
Morphine can be administered through various routes, including oral, intramuscular, subcutaneous, intravenous, spinal cord space injection, or rectal administration. Intravenous administration produces its maximum effect in approximately 20 minutes, while oral ingestion takes around 60 minutes. The duration of its effects typically ranges from three to seven hours. Extended-release formulations, like Kadian, can maintain clinically significant effects for up to 24 hours.
It is widely acknowledged that morphine possesses a significant potential for abuse. Apart from the risk of fatal overdose from single-use, chronic morphine use leads to increased tolerance and physical and psychological dependence, posing substantial harm to the user. Therefore, it is strongly recommended to adhere to harm-reduction practices when using this substance.
| Identifiers | |
|---|---|
| IUPAC name | |
| CAS Number | 57-27-2 64-31-3 (neutral sulfate), 52-26-6 (hydrochloride) |
|---|---|
| PubChem CID | 5288826 |
| IUPHAR/BPS | 1627 |
| DrugBank | DB00295 |
| ChemSpider | 4450907 |
| UNII | 76I7G6D29C |
| KEGG | D08233 |
| ChEBI | CHEBI:17303 |
| ChEMBL | ChEMBL70 |
| PDB ligand | MOI (PDBe, RCSB PDB) |
| CompTox Dashboard (EPA) | DTXSID9023336 |
| ECHA InfoCard | 100.000.291 |
| Chemical and physical data | |
| Formula | C17H19NO3 |
| Molar mass | 285.343 g·mol−1 |
In 1806, German pharmacist’s assistant Friedrich Sertürner achieved a groundbreaking milestone by isolating morphine for the first time.
Throughout more than 50 experiments, Sertürner believed he had successfully extracted the primary active component from opium, marking a pivotal moment as it is generally considered the earliest isolation of an active compound from a plant. This active substance, found to be ten times as potent as opium, was initially named “morphium” by Sertürner, drawing inspiration from Morpheus, the Greek god of dreams, due to its propensity to induce sleep. Merck subsequently commenced commercial marketing of morphine in 1827. While the broader medical community did not immediately recognize the full clinical significance of morphine, it was not until 1831 that Sertürner’s contribution was duly acknowledged, and he received the French equivalent of the Nobel Prize. As the opium plant underwent further analysis, other alkaloids were identified, with one eventually becoming known as codeine. The term “codeine” traces its origins to the ancient Greek word “κώδεια,” referring to a cup shaped like a poppyhead.
The widespread use of morphine was significantly influenced by Dr. Alexander Wood’s invention of the hypodermic syringe in 1853. However, it wasn’t until the American Civil War in 1861, followed by the Prussian-Austrian War in 1866 and the Franco-Prussian War of 1870, that morphine saw extensive application in the field of military medicine. It was during and after these military conflicts that morphine habituation acquired the ominous moniker of the “soldier’s disease” or the “army disease.” Recognizing the addictive and habit-forming nature of morphine, the medical community began searching for a less addictive alternative, which eventually led to the introduction of diacetylmorphine, later marketed as heroin. Ironically, it was later discovered that heroin was not less addictive than codeine but rather the opposite.
The first proposed chemical structure of morphine emerged in 1923, a hypothesis that was subsequently confirmed in 1927 by Robinson and colleagues. Finally, the complete chemical synthesis of morphine was achieved in 1952 by Gates and Tschudi.
Morphine’s primary source is derived from the poppy straw of the opium poppy plant. In 2013, an estimated 523,000 kilograms of morphine were produced, with approximately 45,000 kilograms being directly employed for pain management—an increase fourfold over the past two decades. The majority of this medical usage is concentrated in the developed world. Notably, roughly 70% of morphine serves as a precursor for the production of other opioids like hydromorphone, oxycodone, and heroin.
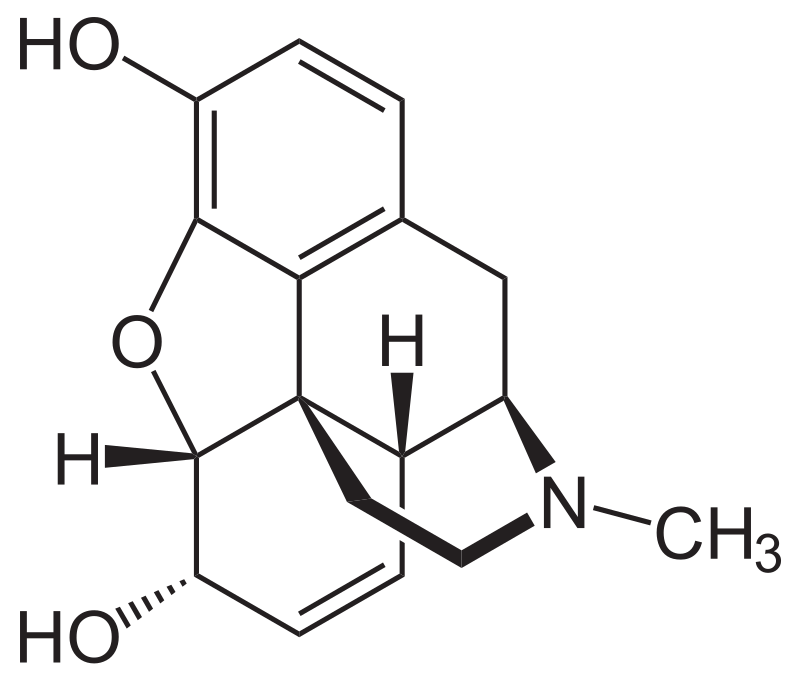
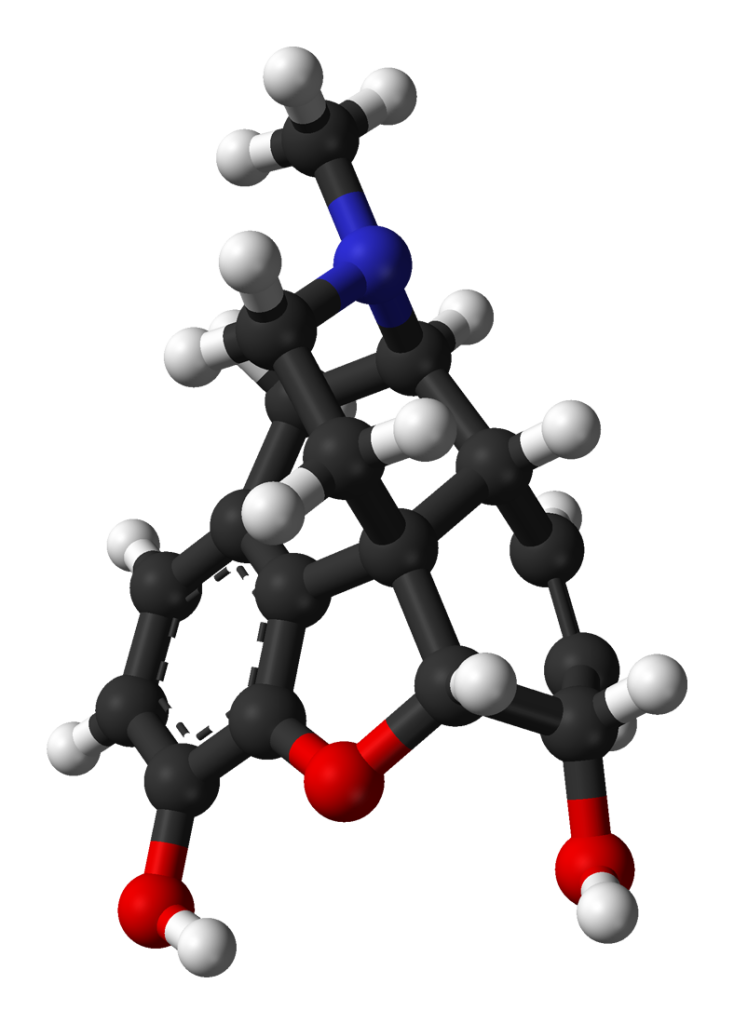
Morphine, classified as a benzylisoquinoline alkaloid, belongs to the morphinan class of opiates. In this chemical family, morphine and its counterparts share a distinctive structural core characterized by three interconnected benzene rings arranged in a zig-zag pattern known as phenanthrene. Additionally, a fourth ring containing nitrogen is fused to the phenanthrene structure at positions R9 and R13, with the nitrogen element situated at position R17 within the combined framework. This fused structure is referred to as a “morphinan.”
Morphine, along with other substances in the morphinan class, features an ether bridge linking two of its rings, specifically connecting positions R4 and R5 through an oxygen group. It possesses two hydroxy groups (OH-) attached at positions R6 and R3 and a methyl group located on the nitrogen atom at position R17.
Morphine serves as a precursor for numerous morphinan-based drugs, playing a pivotal role in the synthesis of codeine through methylation of its hydroxy group at position R3 and in the production of heroin through acetylation. Other closely related opioids, such as hydrocodone, oxycodone, and dihydrocodeine, share structural similarities with morphine. The fundamental chemical structure of morphine serves as the foundational framework for the development of hundreds of opioid derivatives, each with a diverse range of effects.
Morphine exerts its effects by activating three well-known opioid receptors: the κ-opioid (KOP), μ-opioid (MOP), and δ-opioid (DOP) receptors, acting as an agonist. This mechanism of action is rooted in the functional mimicry of the body’s natural endorphins. Endorphins play a crucial role in pain reduction (analgesia), inducing sleepiness and generating sensations of pleasure and enjoyment. These endorphins are typically released in response to various stimuli, including pain, strenuous physical exercise, orgasm, or moments of excitement. By emulating the action of these natural endorphins, morphine delivers its characteristic euphoric, analgesic (pain relief), and anxiolytic (anti-anxiety) effects.
In small amounts, morphine is produced within the human body and serves as an immunomodulator. The endogenous morphine primarily binds to the μ3 opioid receptor.
Metabolism of morphine, hydromorphone, and oxymorphone involves minimal CYP450 enzymatic activity and is instead predominantly facilitated by the action of UDP-glucuronosyltransferases (UGTs), specifically the UG2B7 isozyme. Approximately 90% of morphine undergoes conversion into metabolites, primarily manifesting as glucuronide conjugates: morphine-3-glucuronide (M3G) (45-55%) and morphine-6-glucuronide (M6G) (10-15%). Among these metabolites, M3G exhibits low affinity for opioid receptors and lacks analgesic activity, while M6G binds to the same receptor sites as morphine but exhibits higher affinity and potency.

Please note that the effects listed below are based on anecdotal user reports and the personal analyses of contributors to the Subjective Effect Index (SEI) on PsychonautWiki. They should be approached with a degree of skepticism, as individual experiences can vary widely, and higher doses are more likely to produce a broader range of effects. Additionally, it’s crucial to be aware that adverse effects become more likely with higher doses and may include addiction, severe injury, or even death ☠.
Similar to most opioids, pure morphine generally doesn’t lead to many long-term complications, except for the development of dependence and constipation. The potential dangers associated with morphine use primarily stem from improper administration, overdosing, or the use of impure products.
Using high doses of morphine can result in respiratory depression, which can progress to life-threatening oxygen deprivation (anoxia). This happens because morphine’s interaction with µ-opioid receptors suppresses the natural breathing reflex, with the degree of suppression increasing with higher doses.
Morphine can also cause nausea and vomiting, and some opioid overdose-related deaths occur due to unconscious individuals aspirating on their vomit. This happens when someone unconscious or semi-conscious and lying on their back vomits into their mouth, unknowingly causing suffocation. This risk can be mitigated by ensuring the person lies on their side with their head tilted downwards, a position known as the recovery position.
It is strongly advised to practice harm reduction when using morphine.
Like other opiate-based painkillers, chronic morphine use is highly addictive and can lead to both physical and psychological dependence. When physical dependence develops, abrupt discontinuation can lead to withdrawal symptoms.
Tolerance to many of morphine’s effects, including its therapeutic effects, typically develops with prolonged use. This results in users needing progressively larger doses to achieve the same effects. The development of tolerance to the constipation-inducing effects is particularly slow. Importantly, morphine use can lead to cross-tolerance with other opioids, meaning that after using morphine, other opioids become less effective.
The risk of fatal opioid overdoses significantly increases after a period of abstinence and relapse due to reduced tolerance. To address this, it is safer to take only a fraction of one’s usual dosage if relapsing. Additionally, the environment in which the drug is taken can influence opioid tolerance; studies have shown that familiarity with the environment can impact tolerance levels.
Morphine should not be combined with other depressants, as many reported overdose cases involve interactions with substances such as alcohol or benzodiazepines. These interactions can lead to dangerously high levels of respiratory depression.
Warning: Combining psychoactive substances, even those considered safe on their own, can become dangerous and life-threatening when mixed with certain other substances. Conduct independent research to ensure the safety of combining two or more substances. Some known dangerous interactions include:
Internationally, morphine is categorized as a Schedule I substance in accordance with the Single Convention on Narcotic Drugs. Furthermore, it holds a place on the WHO Model List of Essential Medicines, which comprises crucial medications essential for a basic healthcare system.
1. What is morphine?
2. How does morphine work?
3. What is morphine used for?
4. Is morphine addictive?
5. What are the common side effects of morphine?
6. Can I drink alcohol while taking morphine?
7. How should I take morphine?
8. Can I drive or operate heavy machinery while on morphine?
9. Is morphine safe during pregnancy and breastfeeding?
10. What should I do if I miss a dose of morphine? – If you miss a dose, take it as soon as you remember unless it’s close to the time for your next scheduled dose. In that case, skip the missed dose and continue with your regular dosing schedule. Do not double up on doses.
11. Can morphine be used to treat addiction to other opioids? – Yes, in certain cases, healthcare providers may use morphine or other opioid agonists to help manage opioid addiction and withdrawal symptoms as part of a medically supervised treatment program.
12. Is morphine available over-the-counter (OTC)? – No, morphine is not available over-the-counter. It is a prescription medication and should only be used under the guidance of a healthcare provider.
13. What should I do if I suspect an overdose or have severe side effects? – If you suspect an overdose or experience severe side effects such as difficulty breathing, extreme drowsiness, or loss of consciousness, seek immediate medical attention. In case of overdose, naloxone can be administered to reverse the effects of morphine.
14. How long does the pain relief from morphine last? – The duration of pain relief from morphine varies depending on the formulation and dosage. Immediate-release morphine provides relief for about 4 to 6 hours, while extended-release forms may provide pain relief for up to 12 or 24 hours.
15. Can I stop taking morphine abruptly? – It is important not to stop taking morphine suddenly, especially if you have been using it for an extended period, as this can lead to withdrawal symptoms. Consult your healthcare provider for guidance on tapering off the medication safely.