![]()
Beautiful Plants For Your Interior
Hydrocodone, commonly known as Vicodin or Norco when mixed with paracetamol, is a semi-synthetic opioid morphinan. This compound is synthesized or chemically derived from codeine, one of the opioid alkaloids naturally occurring in the opium poppy. It functions as a narcotic analgesic, typically administered orally to suppress coughs. Moreover, it is frequently taken orally to alleviate moderate to severe pain.
Individuals who use hydrocodone for recreational purposes often report experiencing a profound sense of relaxation and euphoria, particularly at higher doses.
Hydrocodone is primarily prescribed within the United States. According to the International Narcotics Control Board, a staggering 99% of the global supply in 2007 was consumed within the United States.
Much like many other opioids, such as dextropropoxyphene, hydrocodone is frequently combined with acetaminophen (paracetamol). This combination serves the dual purpose of enhancing analgesic effects and deterring potential abuse. However, it’s essential to note that acetaminophen overdoses and prolonged usage, often associated with recreational use, can lead to severe or even fatal liver damage. Presently, the only hydrocodone brand available in the United States without acetaminophen is Zohydro ER, which is offered in doses of up to 50mg.
| Identifiers | |
|---|---|
| IUPAC name | |
| CAS Number | 125-29-1 |
|---|---|
| PubChem CID | 5284569 |
| IUPHAR/BPS | 7081 |
| DrugBank | DB00956 |
| ChemSpider | 4447623 |
| UNII | 6YKS4Y3WQ7 |
| KEGG | D08045 |
| ChEBI | CHEBI:5779 |
| ChEMBL | ChEMBL1457 |
| CompTox Dashboard (EPA) | DTXSID8023131 |
| ECHA InfoCard | 100.004.304 |
| Chemical and physical data | |
| Formula | C18H21NO3 |
| Molar mass | 299.370 g·mol−1 |
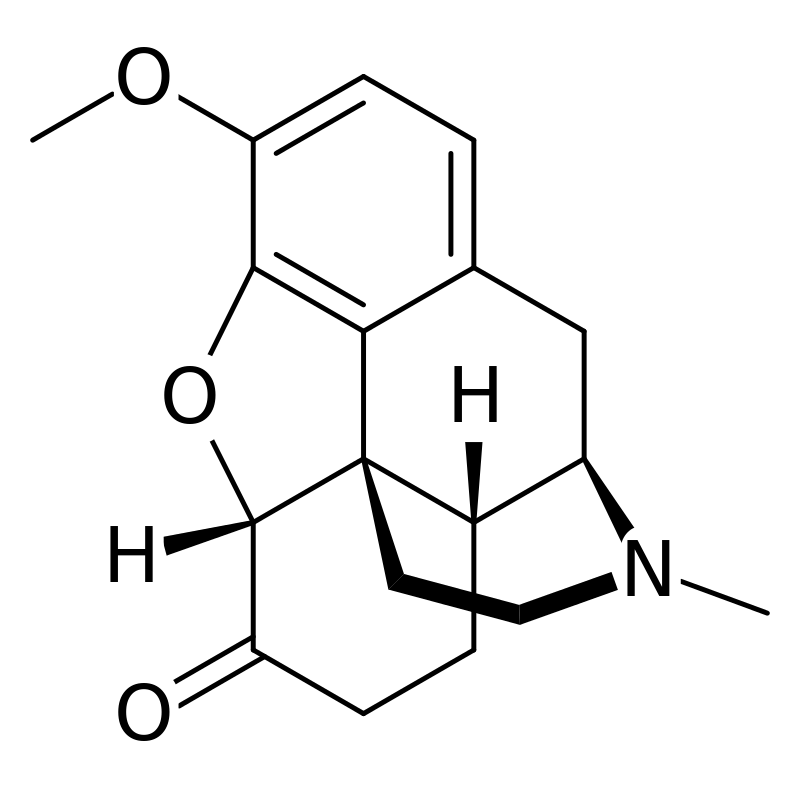
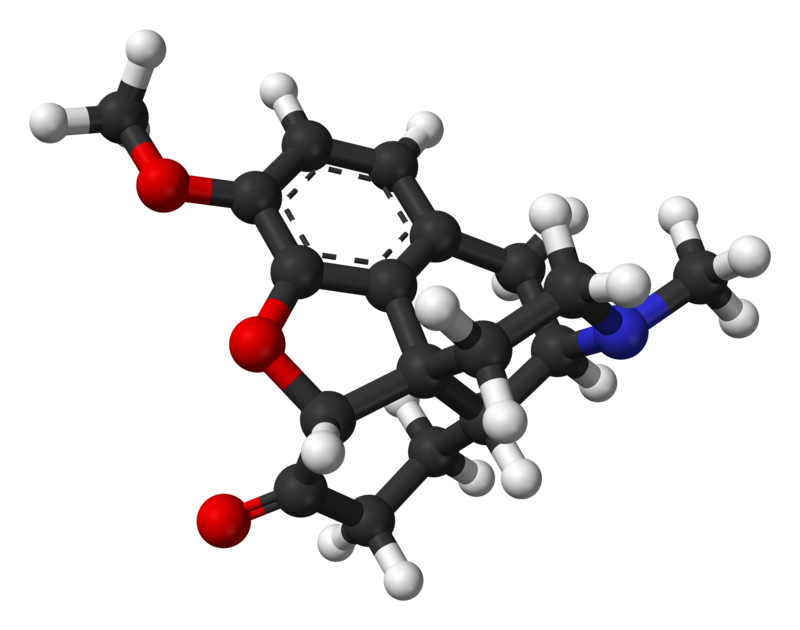
Hydrocodone, scientifically known as 3-methyl-dihydromorphinone, belongs to the morphinan class of opioids. Within this class, hydrocodone and similar molecules share a distinctive structure characterized by a polycyclic core comprising three interconnected benzene rings arranged in a zig-zag pattern known as a phenanthrene. An additional nitrogen-containing ring is fused to the phenanthrene structure at positions R9 and R13, with the nitrogen atom positioned at R17 within the combined framework. This structural configuration is commonly referred to as “morphinan.”
In the case of hydrocodone, and indeed other morphinans, an ether bridge connects two of its rings, specifically linking positions R4 and R5 through an oxygen group. Notably, hydrocodone features a carbonyl group attached to position R6 and a methyl group positioned on the nitrogen atom at R17. Unlike codeine, hydrocodone lacks the double bond on the benzene ring associated with the carbon-oxygen double bond of the carbonyl group.
Hydrocodone also shares the 3-methoxy substitution observed in codeine, with the primary distinction between the two lying in their R6 substituents. Hydrocodone’s structural similarity places it in the same class as other morphinans, including dihydrocodeine, heroin, ethylmorphine, codeine, and oxycodone.
The pleasurable effects of euphoria, anxiety relief, and pain mitigation associated with hydrocodone usage appear to arise from its ability to mimic natural endorphins in the body. Endorphins, responsible for reducing pain, inducing drowsiness, and generating feelings of pleasure, are typically released in response to various stimuli such as pain, rigorous exercise, orgasm, or excitement. Hydrocodone’s capacity to emulate these naturally occurring endorphins gives rise to its therapeutic effects. This mimicry primarily occurs by interacting with μ-opioid receptors, with approximately six times less affinity for δ-opioid receptors.
Inside the liver, hydrocodone transforms into several metabolites. It possesses a serum half-life averaging around 3.8 hours. The hepatic enzyme CYP2D6, a member of the cytochrome P450 family, converts hydrocodone into hydromorphone, which is a more potent opioid.
Interestingly, when hydrocodone is consumed alongside grapefruit juice, there may be an augmentation of its psychoactive effects. This phenomenon is postulated to occur due to the potential interference of CYP3A4 inhibitors found in grapefruit juice with the metabolism of hydrocodone. However, it’s important to note that no substantial research has been conducted to confirm this hypothesis.
Disclaimer: The effects listed below are based on anecdotal user reports and personal analyses from contributors to the Subjective Effect Index (SEI), an open research literature. As such, these effects should be considered with a degree of skepticism.
It is important to note that these effects may not necessarily occur predictably or reliably, although higher doses are more likely to elicit the full range of effects. Additionally, it should be emphasized that adverse effects become increasingly probable with higher doses, including the risk of addiction, severe harm, or even death ☠.
Disclaimer: The following information is based on anecdotal reports and the personal analyses of PsychonautWiki contributors and should be approached with a degree of caution.
Hydrocodone has not shown significant toxicity at reasonable dosages and is generally considered physically benign. However, as with all opioids, long-term effects can vary and may include diminished libido, apathy, and memory impairment. Some individuals may also experience allergic reactions to hydrocodone, such as skin swelling and rashes. It’s crucial to note that at high dosages, hydrocodone can be potentially fatal.
In its pure form, hydrocodone, when taken at appropriate dosages, typically does not lead to many long-term complications aside from the risks of dependence and constipation. Most of the harm associated with opioid use is linked to factors such as inadequate precautions during administration, overdosing, or the consumption of impure products. When hydrocodone is combined with acetaminophen (paracetamol), a common occurrence in pharmaceutical preparations, the safety profile becomes more complex due to acetaminophen’s potential for liver toxicity.
Heavy doses of hydrocodone can result in respiratory depression, potentially leading to dangerous levels of oxygen deprivation (anoxia). This occurs because opioid agonism, particularly at μ-opioid receptors, suppresses the respiratory reflex, with the degree of suppression proportional to the dose consumed. When hydrocodone is co-administered with acetaminophen, the risk of liver toxicity or acute liver failure becomes a significant concern, especially when combined with alcohol. The combined use of hydrocodone and alcohol heightens the risk of severe respiratory depression.
Hydrocodone use, on its own, can also lead to nausea and vomiting, and a significant number of opioid overdose deaths are attributed to aspiration of vomit by unconscious individuals. This occurs when an unconscious or semi-conscious person lying on their back vomits into their mouth, potentially leading to suffocation. To prevent this, individuals must be placed in the recovery position (lying on their side with their head tilted downward) in case of overdose.
In the event of an opioid overdose, it is strongly recommended to administer naloxone intravenously or intramuscularly to reverse the effects of opioid agonism.
Similar to other opioid-based painkillers, chronic use of hydrocodone can lead to moderate levels of physical and psychological dependence. When physical dependence develops, withdrawal symptoms may occur upon abrupt cessation of use. These withdrawal symptoms are primarily somatic.
Tolerance to many of hydrocodone’s effects develops with prolonged use, including therapeutic effects. This leads users to require progressively larger doses to achieve the same effects. The rate at which tolerance develops varies for different effects, with tolerance to constipation-inducing effects developing particularly slowly. After discontinuation, it typically takes 3 – 7 days for the tolerance to decrease by half and 1 – 2 weeks to return to baseline (in the absence of further consumption). Importantly, hydrocodone also presents cross-tolerance with all other opioids, meaning that its use reduces the effectiveness of other opioids.
The risk of fatal opioid overdoses increases significantly after a period of abstinence and relapse due to reduced tolerance. To account for this reduced tolerance, it is safer to take only a fraction of one’s usual dosage if relapsing. Additionally, the environment in which a substance is used can play a role in opioid tolerance, as demonstrated in scientific studies where familiar environments were associated with a lower risk of overdose compared to unfamiliar environments.
Australia: Hydrocodone is classified as a Schedule 8 (S8) controlled drug.
Austria: Hydrocodone is regulated in Austria similarly to Germany (see below) under the Austrian Suchtmittelgesetz (SMG). Since 2002, it has been accessible in the form of German products and those manufactured elsewhere in the European Union, in accordance with Article 76 of the Schengen Treaty.
Belgium: Hydrocodone is no longer authorized for medical use.
Canada: Hydrocodone is categorized as a Schedule I controlled substance and is exclusively available through prescription. It is prescribed both as a standalone medication and in proprietary combinations, often with an NSAID or paracetamol.[citation needed]
France: Hydrocodone is no longer permitted for medical use and is considered a prohibited narcotic.
Germany: Hydrocodone is classified as a controlled substance under Anlage III of the BtMG. It can only be prescribed using a narcotic prescription form.
Luxembourg: Hydrocodone is available by prescription under the name Biocodone, primarily prescribed as a cough suppressant (antitussive) rather than for pain relief (analgesic).
The Netherlands: Hydrocodone is not authorized for medical use and is listed as a List 1 drug under the Opium Law.
Russia: Hydrocodone is classified as a Schedule I controlled substance.
Sweden: Hydrocodone is no longer approved for medical use in Sweden, with the last available formula being deregistered in 1967.[citation needed]
Switzerland: Hydrocodone is specified as a controlled substance under Verzeichnis A. Medicinal use is permitted.
United Kingdom: Hydrocodone is not sanctioned for medical use and is categorized as a Class A drug under the Misuse of Drugs Act 1971. Various formulations of dihydrocodeine, a milder opioid, are frequently prescribed as an alternative.
United States: Effective October 6, 2014, all hydrocodone products are reclassified as Schedule II controlled substances. They are no longer classified as Schedule III narcotics. Prescriptions no longer include refills and a handwritten paper prescription is required for each fill.
1. What is Hydrocodone?
2. How is Hydrocodone typically prescribed?
3. What are the common brand names for Hydrocodone?
4. How does Hydrocodone work?
5. What are the potential side effects of Hydrocodone?
6. Is Hydrocodone addictive?
7. Can Hydrocodone be harmful or fatal?
8. Is Hydrocodone available over-the-counter (OTC)?
9. Can Hydrocodone be used for recreational purposes?
10. What should I do in case of a Hydrocodone overdose? – If you suspect a Hydrocodone overdose, seek immediate medical attention. Naloxone may be administered to reverse opioid effects, but professional medical assistance is essential.
11. Can Hydrocodone interact with other medications or substances? – Yes, Hydrocodone can interact with other medications and substances, potentially leading to dangerous effects. Always consult with your healthcare provider about possible interactions and follow their guidance.
12. Is Hydrocodone legal in my country? – The legal status of Hydrocodone varies by country. It may be controlled, prescription-only, or prohibited. Consult your local laws and regulations or a healthcare provider for information specific to your location.
13. Is Hydrocodone safe during pregnancy or breastfeeding? – Hydrocodone should only be used during pregnancy or breastfeeding under the guidance of a healthcare provider. It may pose risks to the developing fetus or nursing infant.
14. How long does Hydrocodone stay in the system? – The duration Hydrocodone remains in the system can vary from person to person but is typically detectable in urine for up to 2-4 days after use.
15. Can I drink grapefruit juice while taking Hydrocodone? – It’s advisable to avoid grapefruit juice when taking Hydrocodone, as it may interfere with the drug’s metabolism and potentially lead to increased side effects or risks.